

The stages of grief after suicide loss don’t describe what most survivors actually experience. Someone came to our SOS Madison support group a few months after losing a child. They’d done what a lot of people do early on. They’d read about the stages of grief and tried to find themselves in them.
They’d expected to cycle through denial, then anger, then bargaining, then something that eventually became acceptance. But what they were actually living through didn’t look like that at all. Up at 3 a.m. replaying every conversation they’d ever had. Drowning in guilt and shame. Needing, urgently, to understand why. Not moving through a checklist. Feeling like they were failing at grief itself.
I’ve heard some version of that story far too many times in our suicide loss support group in fifteen-plus years of facilitating. Parents, spouses, siblings, friends. Different voices, different losses, same confusion. The grief models they came in with didn’t describe what they were actually living.
That’s not their failure. It’s a limitation of the models themselves. The stages of grief after suicide loss are a particularly poor fit, and the field has been working to close that gap for decades. This post walks through how grief theory has evolved, why the most famous model was never built for people like you, and what newer frameworks by researchers like J. William Worden and John R. Jordan actually say about the grief you are carrying.
If you’re in the early days of this loss or months or years in and still trying to understand why it is so hard, there is a reason. And it’s been studied.
The Model Everyone Knows, and What It Was Actually Built For
Most of us learned about grief through Elisabeth Kübler-Ross. Her 1969 book introduced what became known as the Five Stages of Grief.
- Denial
- Anger
- Bargaining
- Depression
- Acceptance
Those five words are everywhere. They show up in movies and TV. Therapists reference them. Well-meaning friends quote them at funerals and over casseroles in the weeks after a death.
Here is what most people don’t know. Kübler-Ross developed those stages by interviewing terminally ill patients. She was describing what people go through when they are dying. Not what the people left behind experience after a death. The five stages were originally a model for how a person confronts their own mortality, not for how a bereaved person survives someone else’s death.
As the stages spread through popular culture, they were applied to bereaved people in ways Kübler-Ross never fully intended. Researchers who later examined the model found that it had no strong empirical basis for bereavement, that it had moved from being descriptive to being prescriptive, and that bereaved people who didn’t experience these stages in order were being told, implicitly, that they were grieving incorrectly. For suicide loss survivors, the last stage presents its own particular problem: acceptance is not the right word for what healing actually looks like.
Dr. John R. Jordan, one of the leading researchers on suicide bereavement, has described what he calls the “flu model” of grief in our culture. The expectation is that grief is unpleasant but relatively short. You take some time off, people surround you, and then you return to life. Once survivors are back at work and able to smile again, the social signal becomes clear. It’s time to stop grieving.
That model fails most bereaved people. It fails suicide loss survivors almost completely.
Why the Stages of Grief Don’t Match What Suicide Loss Actually Feels Like
The five-stage framework implies a sequence. The word “stages” suggests progression, you get through one, move into the next, reach an endpoint called acceptance. Grief after suicide loss doesn’t work that way. Research going back decades has consistently found that
suicide loss grief is non-linear, often intense, and frequently longer-lasting than grief after other types of death.
What you’re more likely to experience is something that comes in waves. One afternoon you find your footing. Three days later something knocks you flat again. That’s not backward progress. That’s not doing grief wrong. That’s what suicide grief actually looks like.
I’ve written separately about grief ambushes after suicide loss — those moments when grief arrives without warning or invitation. They are among the most common experiences survivors describe, and they happen entirely outside of any staged framework.
The stage model also misses something else.
Grief after suicide loss often carries additional weight that general grief models were never designed to hold.
The guilt.
The unanswered questions.
The shame.
The trauma of a sudden and violent death.
These are not extra stages that arrive after acceptance. They are woven through everything from the beginning.
Worden’s Four Tasks of Mourning: Grief as Something You Do
In the decades following Kübler-Ross, researchers began developing frameworks that tried to describe grief more honestly. One of the most important frameworks came from psychologist J. William Worden. He called his framework the Four Tasks of Mourning, and the word “tasks” was chosen with care. Grief is not something that simply happens to you while you wait for it to end. It is something you actively engage with.
His four tasks are not sequential and have no fixed timeline. You may work on one for months, then find yourself circling back to another you thought you’d already addressed. That is the design, not a failure.
- The first task is accepting the reality of the loss. Not just intellectually understanding that the death happened, but taking it in at a deeper level. For survivors of a suicide death, this task can be complicated by shock, by disbelief, and by the traumatic nature of what happened.
- The second task is working through the pain of grief. Not getting over it. Not bypassing it. Working through it. Worden doesn’t promise the pain will stop. He acknowledges that the pain is the work itself.
- The third task is adjusting to a world without the person who died. This goes beyond the practical changes, though those are real and constant. It includes adjusting to an identity that now contains this loss. The person you expected to be, in the life you expected to have, is not who you are anymore.
- The fourth task is finding an enduring connection with the person who died while embarking on a new life. This is one of the most important shifts in grief theory. Older models often implied that healthy mourning meant letting go and moving on. Worden’s framework, and much of the research that followed, rejected that idea. You do not have to sever your connection to the person you lost in order to heal. You carry them with you, differently, as you build a life forward.
That fourth task resonates with something I hear in our support group. People don’t want to stop thinking about the person who died. They don’t want to move on. They want a way to carry that person into the rest of their lives without being permanently paralyzed by the weight of the grief.
Worden’s fourth task didn’t emerge in isolation. It was shaped by Continuing Bonds Theory, developed by Klass, Silverman, and Nickman in 1996, which formally challenged the assumption that healthy grief means progressively detaching from the person who died. What they found was that maintaining an ongoing internal relationship with the deceased is not pathological. It is normal, and it is often healing. I’ve written about this in Physics = Love: Continuing Bonds After Suicide Loss.
The Dual Process Model: Making Sense of Your Good Days and Bad Days
One of the most practically useful frameworks to come out of grief research in recent decades is the Dual Process Model, developed by Margaret Stroebe and Henk Schut in 1999. It doesn’t replace Worden’s task framework. It describes something different and complementary: the moment-to-moment rhythm of how grief actually moves through a day, a week, a month.
Stroebe and Schut observed that bereaved people don’t grieve continuously. They oscillate.
- Loss-orientation is the mode of sitting directly with grief: thinking about the person who died, feeling the absence, crying, remembering.
- Restoration-orientation is the mode of rebuilding: getting through the day, handling practical demands, adapting to new roles. Both modes are necessary. Neither is a failure.
What this model explains, better than any other framework, is why a good Tuesday can be followed by a devastating Wednesday without that meaning you are going backward.
The movement away from grief is not avoidance. It is recovery so you can turn toward the grief again.
For suicide loss survivors this model carries particular relief. Many survivors feel guilty when they have a good hour or a good day, reading it as forgetting the person who died. The Dual Process Model says something different. The moment of laughing at dinner is not betrayal. It is restoration-orientation doing its work, giving you the capacity to return to the grief when it comes back.
Why Grief After Suicide Loss Is Different From Every Other Kind
You may have heard that loss is loss. You may have felt you should be doing better than you are right now. The research says something different. Grief after suicide loss carries distinct features that set it apart from bereavement after illness, accident, or other causes of death.
As I’ve described in anticipated versus unanticipated loss, suicide loss is almost always unanticipated. That shock layer adds weight to everything that follows. But even among sudden, traumatic losses, suicide loss carries particular features that research has documented over and over.
The search for why. Most survivors of suicide loss are consumed, especially early on, by the need to understand what happened.
This is not morbid curiosity. It is the mind’s attempt to make sense of something that has no ready explanation. That search can go on for years. Some answers come. Many never do. The quest for understanding why is one of the defining experiences of this grief.
Two posts go deeper into what was happening in the person’s mind: why they couldn’t just tell you when they were in crisis, and the suicidal trance state that made death feel like the only exit. Reading those posts doesn’t answer the why. But for many survivors, understanding what was actually happening in the person’s mind shifts something in the weight of the guilt.
Beyond the search for why, research has identified three other features that show up consistently in suicide loss grief and rarely in other forms of bereavement.
- Guilt and felt responsibility. Research has consistently found that survivors of suicide loss experience higher levels of guilt and self-blame than people bereaved by other causes of death. The replaying of conversations. The “what ifs.” The certainty, in your worst moments, that you should have seen it coming or done something differently. That guilt is one of the most persistent things survivors carry, and you are not alone in it.
- Stigma and shame. There remains a stigma attached to death by suicide that does not exist for other causes. That stigma shapes how survivors talk about the death, who they tell, and where they feel safe reaching for support. Research has found that survivors of suicide loss are more likely than other bereaved people to feel the need to conceal the cause of death. That isolation adds to an already heavy burden.
- Trauma. A death by suicide is typically sudden and may involve violent circumstances. The combination of shock, trauma, and grief creates a burden that is qualitatively different from grief following an anticipated death or a natural one. For many survivors, this grief has a physical dimension. It lives in the body, not just the mind.
The Jordan Framework: Grief Research Built for Suicide Loss Survivors
If there is one researcher whose work has done the most to establish suicide bereavement as its own field of study, it is John R. Jordan. His 2001 paper in Suicide and Life-Threatening Behavior established that suicide grief was qualitatively distinct from other bereavement in three dimensions: the thematic content of the grief (guilt, shame, the search for why, the feeling of having been left), the social processes surrounding the survivor (stigma, isolation, the pressure to conceal), and the impact on family systems. The post on surviving suicide loss as a family goes deeper into that third dimension.
In 2020, after nearly forty years of clinical work with survivors, Jordan published Lessons Learned: Forty Years of Clinical Work With Suicide Loss Survivors in Frontiers in Psychology. It is the accumulated wisdom of a lifetime spent in the room with people carrying exactly what you are carrying.
Perceived intentionality: the wound at the center
Jordan identifies perceived intentionality as the element that most distinguishes suicide loss from every other form of grief. Most survivors experience the death as a voluntary choice. That perception, even when survivors understand that mental illness and unbearable pain drove it, activates something no other loss produces: the feeling of having been left on purpose. It is why the guilt cuts deeper here than in other losses, and why the “why” question is so consuming. Someone who died of a heart attack did not choose to leave. The post Is Suicide a Choice? goes deeper into the complexity Jordan himself acknowledges, that the question is not simple, and that understanding it differently can shift the weight of the guilt. The Suicide Prevention Resource Center and the American Foundation for Suicide Prevention have both built survivor resources around this understanding.
Closely related is what Jordan calls the “responsibility” question: who is accountable for this death? Most survivors begin by blaming themselves, cycling through what he describes as the “if-onlys.” If only I had called that day. If only I had insisted on more help. If only I had known.
Jordan’s clinical experience is that this self-blame is almost universal in early grief, and it is one of the most important things for a clinician or a peer facilitator to understand about what survivors are carrying.
Hindsight bias is the specific cognitive pattern underneath the if-onlys, and understanding it can begin to loosen the grip of that self-blame.
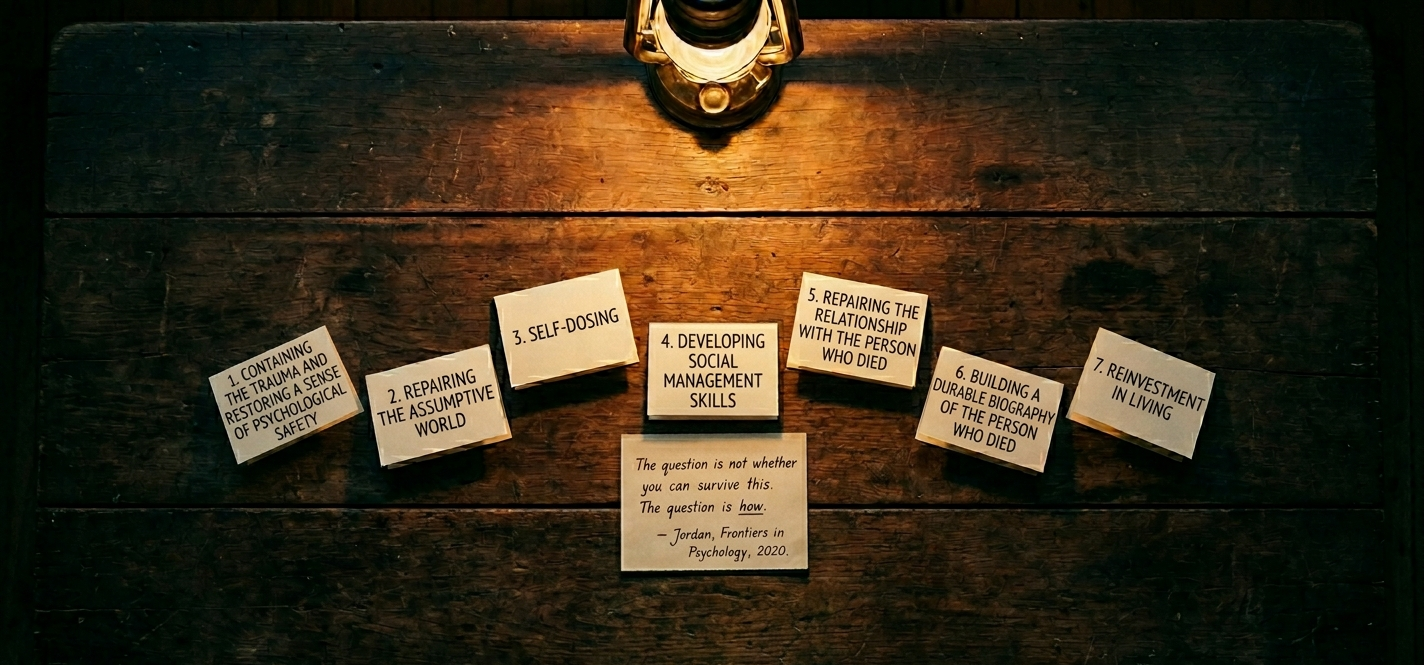
The seven tasks of psychological integration
The 2020 paper moves beyond describing what makes suicide grief different and into what healing from it actually requires. Jordan outlines seven tasks of psychological integration, not stages, not a sequence, but a set of things that most survivors need to work through in order to carry this loss forward.
- The first task is containing the trauma and restoring a sense of psychological safety. Many survivors develop trauma symptoms, intrusive memories, the need to avoid anything that might trigger a reliving of what they found or imagined. Jordan is direct that these symptoms need specific clinical attention, not just general grief support.
- The second task is repairing the assumptive world. Every person carries implicit beliefs about how life works: that the world is predictable, that loved ones can be kept safe. A suicide death shatters those beliefs without warning. Healing requires building a new set of assumptions that are honest about what happened while still allowing a person to function and trust again.
- The third task is what Jordan calls self-dosing, learning to regulate the intensity of grief rather than being controlled by it. This is where he explicitly connects his clinical framework to the Dual Process Model. The goal is to develop the ability to move between loss-orientation and restoration-orientation with increasing intentionality, so that grief becomes something you engage with rather than something that ambushes you.
- The fourth task is developing social management skills. A suicide death strains relationships in specific ways. Other people don’t know what to say. Within families, different people may need incompatible things at the same time. Survivors often need language and skills for navigating these dynamics that they have never needed before.
- The fifth task is repairing the relationship with the person who died. Jordan draws directly on Continuing Bonds Theory here. Suicide can rupture that relationship, leaving survivors with a sense of betrayal or abandonment that needs to be addressed, not bypassed. The work is finding ways to continue an internal dialogue with the deceased and transform the relationship into a form that can be carried forward.
- The sixth task is building a durable biography of the person who died. Suicide can reduce a person’s entire life to the manner of their death. Jordan names the deliberate work of reclaiming the whole story of who they were as a specific healing task, one that often requires the support of others who knew them.
- The seventh task is reinvestment in living. Jordan is clear that exposure to suicide increases a survivor’s own risk, and that part of what healing requires is consciously choosing reasons to continue. Not pretending the grief is over. But finding, over time, reasons to be here.
I’ve had the privilege of sitting in AFSP’s Facilitating a Suicide Bereavement Support Group training, , taught by Jordan himself. The room was full of facilitators and counselors, and I watched something shift in people as they worked through the material. His framework gives language to things survivors already knew in their bones but couldn’t articulate.
The 2020 paper ends with a section on post-traumatic growth, Jordan documents that many survivors, over time, develop a changed outlook on life, greater resilience, and a deepened capacity for compassion. Not because the grief went away. Because they carried it and found they were capable of more than they knew.
Jordan has also been clear about something that matters if you are in early grief and wondering whether what you are experiencing is normal. The research does not show that every survivor ends up with serious complications. Many people carry this grief and find their way through it.
But suicide loss survivors are at higher risk for prolonged grief, for post-traumatic stress, and for depression than people bereaved by other causes.
Prolonged grief disorder is not grief that simply hurts for a long time. It is grief that remains severe, largely unchanged, and significantly disabling beyond twelve months after the loss, interfering with daily functioning in ways that go beyond the expected course of bereavement. It is distinct from depression, though the two can occur together, and it has its own clinical profile and specific treatment approaches. Research has found that survivors of suicide loss develop prolonged grief at roughly four times the rate of the general bereaved population. A dedicated post on prolonged grief disorder is coming that will go much deeper.
You are not experiencing something unusual if this grief is difficult. You are experiencing something that is, statistically, more likely to be difficult for survivors in your position.
Questions Survivors Ask About Grief Models and Suicide Loss
- Am I doing grief wrong if I don’t go through stages in order?
No. The stage model was never an accurate description of how most bereaved people experience grief, and it was never designed for grief after suicide loss. What you’re going through, non-linear and hard to predict, is entirely consistent with what the research actually shows. You are not failing at grief. - Why does my grief feel so different from what people around me seem to be experiencing?
Because grief after suicide loss carries features that are qualitatively different from other types of bereavement. Researchers including Jordan have documented over decades that this grief tends to carry heavier guilt, a more intense search for why, and a greater burden of stigma and shame than grief after other causes of death. Your grief feeling different from those around you is not weakness. It reflects the specific nature of this particular loss. - Why can’t I stop replaying everything I should have done differently?
Jordan calls this the “if-onlys,” and he describes it as nearly universal among suicide loss survivors in the early period of grief. Most survivors begin by blaming themselves, cycling through a litany of things they wish they had said, done, or noticed. This is not a sign of actual guilt. It is the mind’s attempt to find a version of events where the death could have been prevented, because that is less unbearable than the alternative. Understanding that this pattern is documented and expected does not make it stop, but it does mean you are not uniquely broken for experiencing it. - Why does the world feel unsafe and unpredictable in a way it never did before?
Jordan’s 2020 paper calls this the shattering of the assumptive world. Most people carry implicit beliefs: that life is somewhat predictable, that someone in serious pain would reach for help, that paying close attention keeps loved ones safe. A suicide death demolishes those beliefs without warning. One of Jordan’s seven integration tasks is specifically about rebuilding them. The disorientation you are feeling is not weakness. It is a rational response to having those foundations removed. - Is it actually possible to build a meaningful life after this?
Jordan addresses this directly in his 2020 paper. He documents post-traumatic growth among many suicide loss survivors: a changed outlook on life, greater resilience, and a deepened capacity for compassion. Not because the grief went away, but because survivors carried it and found they were capable of more than they knew. That is what the research shows is possible, and it is what many survivors who have been sitting in support groups for years have lived.
What the Stages of Grief Research Means for You Right Now
If you’re reading this in the early days of this loss, or months or years out and still trying to understand what’s happening to you, here is what I want you to take from this.
You are not doing grief wrong. The fact that your grief doesn’t look like five orderly stages is not evidence of failure. It is evidence that you are a human being responding to a traumatic, unexpected loss in the way human beings actually respond to those losses.
Worden’s framework tells you that grief is active and non-linear. Jordan’s framework tells you that your grief has specific, documented features that distinguish it from every other kind of loss, studied and recognized for decades. You are not inventing this. You are not alone in it.
One of the most consistent findings in suicide bereavement research is that peer support among other suicide loss survivors is among the most effective forms of support available to you. Being with people who have this particular grief changes something. You stop explaining yourself. You hear your own experience reflected back, and it becomes, a little at a time, more bearable. The AFSP support group finder and the Alliance of Hope for Suicide Loss Survivors can both help you find that kind of community.
When you search through AFSP, listings that note the facilitator has completed AFSP’s Facilitating a Suicide Bereavement Support Group training as a signal someone trained specifically in the grief this post describes, not general bereavement support.
Peer support and individual therapy are not in competition. Many survivors benefit from both. If you are not sure whether working with a counselor is the right step for you, the post Suicide Loss and Therapy helps you think that through honestly. When you are ready to look, Finding a Grief Counselor After Suicide Loss: A Practical Guide walks through what to look for, what questions to ask, and why finding someone with specific experience in suicide bereavement matters.
These frameworks don’t promise a neat path through. They don’t tell you when you should be better. They tell you that this is real, that it is hard, and that adaptation, not resolution, is what healing actually looks like.
When I lost my son John in 2009, I didn’t know any of this. I just knew that what I was feeling didn’t fit any map I’d been given. Finding other survivors, people who understood this grief from the inside, was the first thing that actually helped. Not because they had answers. Because they had the same questions.
You don’t have to have it figured out yet. You just have to stay.
Posts You May Also Like
- Two Different Roads: Understanding Grief in Anticipated and Unanticipated Loss – Explores why the sudden, unexpected nature of suicide loss hits differently than grief you had time to prepare for.
- Grief Ambushes After Suicide Loss: When Grief Catches You Off Guard – Looks at those unexpected moments when grief arrives without warning and what to do when they happen.
- Suicide Is Not About a Desire to Die: Understanding Psychache – Helps survivors understand what was driving the pain behind the death, which can shift some of the guilt and the “why.”
- Suicide Crisis Syndrome: Why They Couldn’t Just Tell You – Explains the acute mental state that precedes many suicide deaths, which can help survivors understand why the person didn’t reach out or seem to be in crisis.
- Suicidal Trance: What It Means for the Questions You Still Carry – Looks at what survivors can understand about the person’s state of mind, and how that understanding relates to the guilt and unanswered questions you carry.
PRINTABLE GUIDE PDF
A four-page PDF guide has been generated for survivors to print, save, or share.
Leave a Reply